Introduction to Quality Improvement
Improvement in Healthcare
Healthcare systems are complex, inefficient, unreliable and error prone. Everyday, healthcare workers experience difficulties working within these systems as they attempt to complete their duties. Problems arise and the quality of healthcare provided is impacted. But the problems are not a mistake, rather they are the result of a system perfectly designed to generate them. The only way to address the problems and improve the quality of healthcare delivered is to change the system.
Healthcare should be available to all regardless of race, gender, wealth, education or location. Our goal is to safely and efficiently deliver modern medicine to all who would benefit from it. It is too easy to hold your hands up and give in to the status quo. Instead, you can get involved and make a difference by changing the system from within. This is where quality improvement methodology comes in. As well as delivering healthcare, it is our duty to improve the system that governs our actions.
Staff on the frontline know where the real problems are. Take a moment and ask colleagues about five things they do every day that doesn’t work. These are problems that need to be fixed! In an ideal organisation, everyone should be using quality improvement methods all of the time as part of their normal working day. No single change is ever 'the thing’ that results in improvement, but the changes you make are ever so important.
Six Dimensions of High-Quality Healthcare
In 2001 the Institute of Medicine (USA) published a report entitled Crossing the Quality Chasm: A New Health System for the 21st Century. This report examined the reported differences between good healthcare and the healthcare Americans were actually receiving. It identified six dimensions for improvement, and these have since become the six aims of quality improvement in healthcare.
Safe
- We should not harm people nor add to the burden of illness. We must reduce the risks and hazards from the care itself.
Effective
- We should offer forms of medicine that are known to help while avoiding the use of medicines that do not help. Our care should be driven by our scientific knowledge.
Timely
- Delays are harmful and costly to patients. Needless delays should be reduced.
Patient Centred
- We should be respectful and responsive to individuals. Patients should be in control of their own care and make decisions about what affects them.
Efficient
- We should avoid wasting equipment, supplies, ideas and energy.
Equitable
- Care should not vary in quality because of personal characteristics.
Roots within Industry
The idea of continuous improvement originated in the early 20th century with Walter Shewhart and his student William Deming. As traditional craftmanship moved towards mass production and automation techniques, quality became an important issue for factories across the globe. A statistician named Walter Shewhart developed methods for assessing the quality of manufactured products and described ways to improve the manufacturing process to enhance quality. This included the use of statistical process control and the Shewhart cycle (plan-do-study-act). The result was a shift from inspection of end products to the monitoring and adjustment of the processes which produced them.
William Deming first encountered the ideas of continuous improvement while he worked alongside Shewhart as his assistant. They continued to refine the methodologies together. Deming further developed the notion of continuous improvement and brought it into non-manufacturing processes, including clerical and administrative activities. He was an avid teacher and ran courses for both engineers and students on these methods. He called his theory of management and improvement the System of Profound Knowledge.
Following the Second World War, Deming began lecturing the Japanese on these statistical methods and the importance of company-wide quality, a combination now known as Total Quality Management. His ideas were widely incorporated into post-war Japan as they sought to improve the quality of their own goods and reduce the wastage of scarce raw materials. By the late 1970s Japan had become a leader in quality manufacturing leading to the recognition of the ideas of Shewhart and Deming across America. It is from these roots that modern improvement in healthcare began.
Theories and Models in Healthcare
Model for Improvement
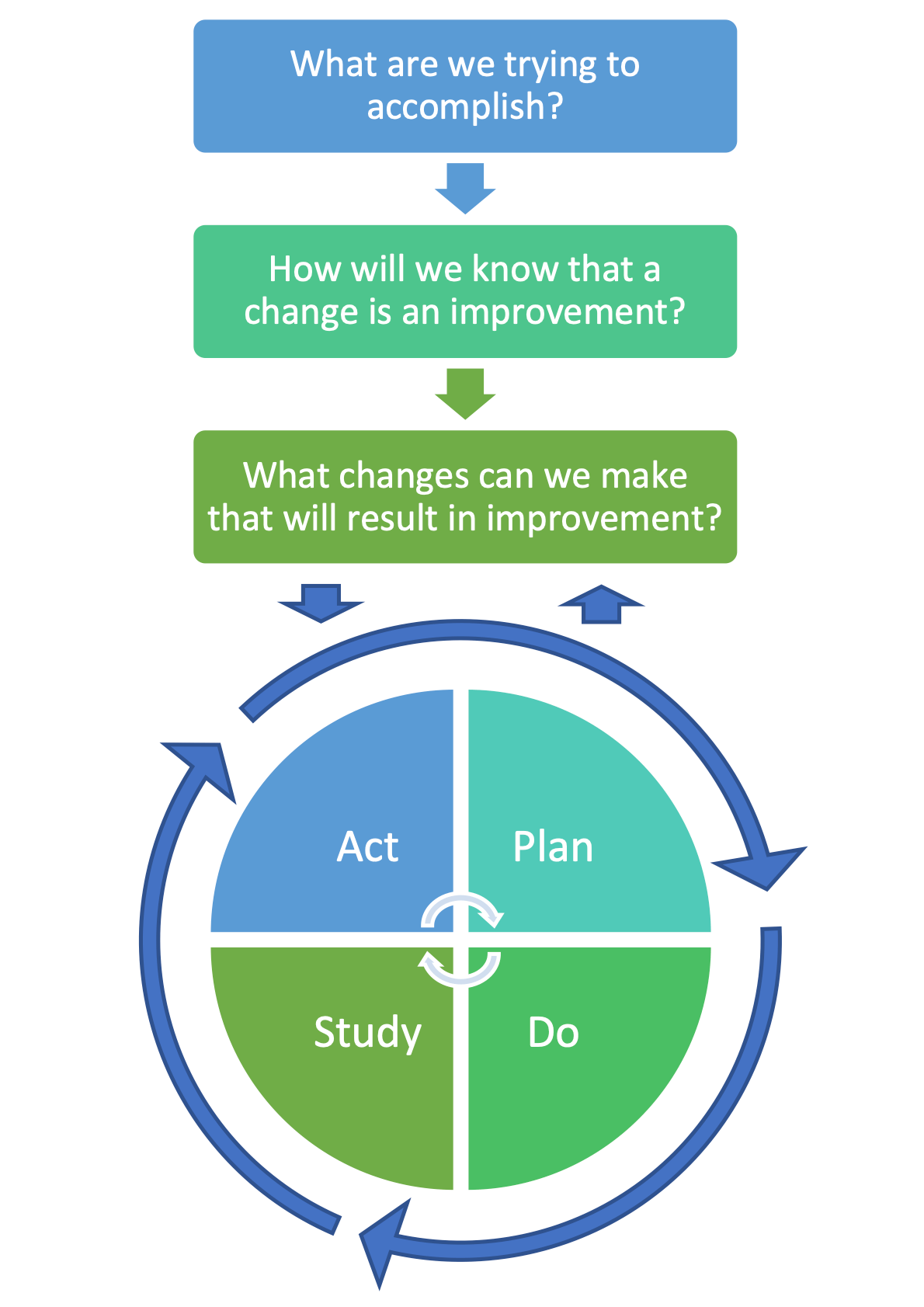
The Model for Improvement was developed by the Associates in Process Improvement and is now the most widely used model within healthcare. It was designed to accelerate improvement within organisations and is outlined in the diagram below. The first part consists of three short questions which systematically evaluate the problem and identify potential solutions, while the second part outlines the steps for testing the change idea in the real world. The cyclical nature of the model allows the change to be refined and improved through repeated cycles of testing and learning.
Four Phases of Improvement
Every improvement project goes through four distinct phases. These are:
Innovation
- Find out what really frustrates people and then help them find a solution.
- Create an aim statement and define your data collection plan.
- Generate new ideas for change.
Pilot
- Test a change on a small scale using a PDSA cycle and adapt to improve results.
- Increase the scale and scope of tests as our degree of belief in the innovation increases.
Implementation
- Make the change a new standard process in one setting.
- Continue testing with PDSA cycles involving more people, time and resources.
- Promote adoption of the innovation.
Spread
- Implement the change in several settings/locations or share the innovation across a network.
- Incorporate the change into routine work, stabilise the gains and spread the innovation as the new normal.
- Often performed by the senior management team.
More on the Pilot Phase
Pilots involve small numbers of people, encounter less resistance to change and are not intended to make the change idea permanent. They involve rapid testing cycles which slowly increase in scale and scope. Failure is commonly encountered, and this provides valuable opportunities to learn from mistakes.
More on the Implementation Phase
The ultimate goal of an improvement project is for your change idea to become a permanent part of the process. This occurs during the implementation phase following the development, testing and refining of changes achieved through several PDSA cycles under a variety of conditions. You should have a high degree of belief that your change will result in improvement and your tolerance for failure should be low. Implementation takes time and will also require support processes to ensure the change is being maintained. Change can be said to be established once 100% of staff turnover and the change remains in place.
Theories and Models from Industry
System of Profound Knowledge
Created by William Deming, the System of Profound Knowledge is based on the idea that each organisation is composed of a system of interrelated processes and people. The success of all workers within the system is dependent on the ability of management to balance each component in order to optimise the entire system. This theory of improvement emphasises the importance of quality over production. It is comprised of four components through which the world is simultaneously viewed:
Appreciation of a System
- What is the whole system that you are trying to manage?
- How do the different parts interact with and rely on one another?
Knowledge about Variation
- What is the variation in results trying to tell you about the system?
- Why did something go wrong?
- Why are results so poor?
- How can you repeat successful results?
Theory of Knowledge
- What are your predictions about the system’s performance?
- What are the theories that form the basis for these predictions?
Knowledge of Psychology
- What are the important interactions among people in the system?
- How do people in a system react to change?
- What motivates people to act as they do?
When assessing a system, you start with a theory of how it performs. This theory is a prediction, not an explanation. The theories are developed, applied and tested and this leads to increasing knowledge. Beware, a theory can only be proved incorrect; it can never be shown to be true. Remember, the system is a network of interdependent components that work together to try and accomplish an aim. Action within one part of the system will directly affect the system in other areas. Similarly, the different world views people possess will directly influence their behaviour and therefore how the system works. Leveraging human behaviour helps us to understand and accelerate change. Finally, there are two types of variation: a change can be significant (special cause variation) or random noise (common cause variation). Understanding the difference enables you to know if your change is having a beneficial effect.
Six-Sigma
A six-sigma process is defined as a process in which 99.99966% of all parts are statistically expected to be free of defects. Essentially, it is about reducing the variation (defect rate) in products. It relies on the idea that manufacturing and business processes have characteristics that can be defined, measured, analysed, improved and controlled. A stable and predictable process can be achieved through continuous efforts to reduce process variation. Commitment from the entire organisation is required to meet this goal. There are two different methodologies for achieving this. One example is the DMAIC Method:
- Define
- Define the system, customer, customer needs, project goals.
- Measure
- Measure key aspects of the current process and collect relevant data.
- Analyse
- Analyse the data to investigate and verify cause-and-effect relationships. Seek out the root cause of the defect under investigation.
- Improve
- Improve the current process based on data from analysis by running tests of change.
- Control
- Control the future process to ensure that any deviations from the target are corrected before they result in defects.
Lean Manufacturing
This is a production method derived from the operating model of Toyota. It seeks to continually and incrementally improve the product and process while eliminating redundant activities (i.e. reduce wasted time and resources). An activity is deemed value adding only if the customer is willing to pay for it. Everything else is waste and should be eliminated, simplified, reduced or integrated. Lean manufacturing is based upon five key principles:
- Value
- Specify the value desired by the customer.
- The Value Stream
- Identify the value stream (the set of actions that take place to add value to a product) and challenge all of the steps currently necessary to provide it.
- Flow
- Make the product flow continuously through the remaining value-added steps without interruptions or delays.
- Pull
- Introduce pull between all steps where continuous flow is possible. This means preparing the right number of products just-in-time for when they are needed.
- Perfection
- Make continuous process improvement a part of the organisational culture. Every employee should strive for perfection while delivering products based on the customer needs. Consequently, the number of steps and the amount of time and information needed to serve the customer should continually fall.